

Managing Risks Associated with Structured Medication Reviews
Dr Duncan Petty is an independent pharmacist who researched structured medication reviews for his PhD. He works in General Practice as well as being a non-executive director for a GP Federation. Dr Petty led a webinar about managing risks associated with structured medication reviews. This blog post is taken from his webinar. Structured Medication Reviews are both topical and important. Here at MORPh, we are keen to support primary care and PCN pharmacists to improve their confidence in conducting SMRs. We hope you will find this post useful and for more information on the topic, check out our upcoming webinar training. We have regular, free sessions on Structured Medication Reviews, including managing risk.
Structured medication reviews: Managing your own risks as a primary care pharmacist
Things we can do to manage risk:
- Education and training: Learning from webinars, learning the skills in practice and seeking feedback. It is easy to become professionally isolated in practice so it is useful to seek feedback from colleagues such as nurses, GPs and other practitioners where possible.
- Work within your level of competence: Know that you are competent and get feedback to work out where your competence level is
- Know when to seek help
- Documentation and record keeping: Important for handing over care and seeking advice
- Don’t try to be an expert on everything but act as an advocate for one patient

Times that can be particularly risky for patients
We have all experienced an increased level of risk due to the pandemic. The frail elderly in particular have become more isolated, which increases their level of risk. We need to get back to seeing people face to face where possible. Particularly risky times for patients include:
- After discharge from hospital: We need to be proactive, particularly with the frail elderly to make sure that they understand what is happening and that they are on the correct medicines and can get access to them
- Patients new to your list before notes arrive: You would be adding to the prescription blindly. Try to get notes as soon as possible, prescribe smaller doses to start with. People who often change lists may be seeking addictive medicines when their previous pharmacist has said no, which is something to be aware of.
- Signing repeat prescriptions that are not yours: We should not be block-signing repeat prescriptions as pharmacists. It is important not to sign anybody else’s prescriptions unless we are sure that they are correct.
- Temporary residents: Are they asking for something they need or seeking addictive medication?

Clinical documentation of structured medication reviews
Pharmacists are not necessarily taught how to document things, but it is something we do all the time. Reasons why it is important:
- Improved accountability
- Helps to address complaints and legal processes
- Helps to identify risks, therefore enabling early detection of complications
- Makes continuity of care easier
- Provides documentary evidence of services delivered
- Promotes communication and information sharing between the multidisciplinary team (MDT)
- Records how decisions relating to a person’s care are made
- Supports service delivery
- Helps to make effective clinical judgments and decisions
- Supports care and communication
- Helpful for clinical audit, research, resource allocation and performance planning
SBAR communication tool
SBAR is a communication tool that was originally designed by US Navy Submarine Commanders. They needed to communicate clearly and concisely to avoid disaster. The American health service then started to use SBAR and the NHS have followed suit and started to recommend it. It is easy to use, structured communication and makes you think about what you are asking for, so that the person you are communicating with understands what you are asking of them. SBAR Communication takes the following form:
- SITUATION: Who you are, what you are calling about and why
- BACKGROUND: When and why the patient was admitted, what procedures they have had, change to their condition, their last set of observations, their normal condition
- ASSESSMENT: What you think the problem is, what you have done or that you are unsure of the problem and why you need help
- RECOMMENDATION: What you need the person you are communicating with to do and any questions, e.g., what should you do in the meantime?

Structured medication reviews for patients nearing the end of life
There are three triggers that suggest people may be nearing the end of life:
- People with cancer nearing the end of life who tend to have a fairly rapid decline
- People with COPD, heart failure and organ system failure who decline gradually and become more frail after being in bed in hospital for a few days
- Frail elderly who may have co-morbidities such as COPD and they show a very gradual decline
Around the deprescribing and structured medication review agenda, we need to focus on the frail elderly. As they decline, their needs change and we have to look at quality of life rather than quantity. We need to learn to have difficult conversations with people about stopping medicines because they are unlikely to benefit from them. Patients may think you are just trying to save money when in reality you are trying to make their final years of life better. It is a skill to have a conversation around this difficult topic in the final years of their life.
Care home patients
Many care home residents are often frail elderly with many comorbidities. They may fall into the following categories:
- Multiple morbidities
- Lack autonomy
- Towards the end of life
- Have different care priorities
- May not be able to engage in shared decision making
- Often on multiple medicines – in a care home review, most people will need at least a 10% medication reduction and probably more
- Medicines that were once useful may no longer be helpful, e.g. statins
- Older people often handle medicines less well
- There may be poor systems for medication review in care homes
- Administration errors are relatively common in care homes

Identifying medicines that may need to be deprescribed
Here are some useful resources that pharmacists can use to back up their decisions on stopping medicines.
- Beers criteria: An explicit tool that lists things that are not good for older people
- Check lists: Such as the medication appropriateness index to remind you what to look at when considering deprescribing (an implicit tool)
- STOPP/START: An explicit tool that gives you an indication of medications that indicate a higher risk of hospitalisation. STOPP criteria searches can be imported to your system if you have System One. This gives you a list on each patient of what STOPP criteria medicines apply to that person. This is a good starting point for SMRs.
- STOPP Frail: An explicit tool – a more abbreviated version of the STOPP criteria, categories of medicine to look out for that may need deprescribing or reducing.
- Medstopper: An explicit tool found at medstopper.com – gives you an indication on when it may be worth stopping a medication in certain situations.
Structured medication reviews: Polypharmacy guidance
The Polypharmacy Guidance is available online. It lists potentially unnecessary drug therapy that may be risky to patients. It is a good way to check expired indications – where it was once useful, but it is not anymore and people may be left on tablets that they no longer need. For example, this often happens with iron tablets. There may also be medicines that have been prescribed incorrectly in the first place.
The Polypharmacy Guidance contains a benefit versus risk section. Certain tablets may be worth reviewing in the patient’s current circumstances, having been prescribed when they were more active or living a different lifestyle. These need to be reviewed in collaboration with the patient with a follow-up review scheduled in.
Capacity to make decisions
It is important to understand the Mental Capacity Act 2005, as detailed in Making Decisions: A guide for people who work in health and social care. In summary, these are the five principles of capacity:
- Every adult has the right to make their own decision and must be presumed to have capacity to do so unless it is proved otherwise
- People must be supported as much as possible to make a decision before anyone concludes that they cannot make their own decision
- People have the right to make what others might regard as an unwise or eccentric decision
- Anything done on behalf of a person who lacks mental capacity must be done in their best interests
- Anything done for or on behalf of people without capacity should be the least restrictive of their basic rights and freedoms
Barriers to deprescribing
Deprescribing is difficult and there are many barriers that may stand in our way. Understanding the barriers is the first step in overcoming them. Barriers may include:
- Poor awareness and insight into the problem – believing one thing and acting in a different way.
- Inertia – fear of negative consequences makes us more likely to do nothing. To overcome this, it is helpful to engage the patient and relatives in the decision-making process and document it well.
- The drug seems to work with few side-effects
- Prescribing meets patients’ needs so it is difficult to stop and will require follow-up consultations which we don’t have time for
- Devolvement of responsibility – e.g., that the drug was started by the hospital so they should stop it – which is not necessarily possible if they have been discharged
- Self-efficacy – not having the confidence to do it
- Lack of evidence and incomplete clinical picture
- No helpful guidelines as guidelines always help us to prescribe and rarely give us evidence to help us to deprescribe – few NICE guidelines even mention stopping medicines
- Feasibility
- Ambivalence
- Resistance to change or perception that a patient may be resistant to change
- Time and effort involved
- This is the way we’ve always done it – work practices and culture
Patients’ barriers to deprescribing
As well as our own barriers to deprescribing, we need to look out for patients’ barriers. These may include:
- Unintentionally withholding information about adverse drug events as they attribute them to ageing
- Patient characteristics such as cognitive impairment, functional dependency, level of education and old age hinder a patient’s explanation of problems
- May not wish to stop familiar medications
- Patients’ demands, wishes and expectations and those of their families
- Reluctance of prescriber to talk to patients about their life expectancy
It is important to manage expectations before starting on a medication. For example, let them know whether it is a short course of medication, what it is likely to achieve and whether it is a trial. You may even want to avoid the prescription in the first place. For example, antidepressants may not be needed for mild depression and opiods definitely shouldn’t be used for back pain.
When to do a deprescribing review
- Deprescribing should always be considered when new things are being added to the repeat list
- When medical or social circumstances change, deprescribing should always be considered. For example when a person moves into a higher level of care, starts to fall, can no longer swallow or has limited life expectancy
- When a person’s morbidity burden increases due to worsening conditions, new conditions, increasing frailty or decreasing kidney function
- At the request of the patient
Defending the decision to deprescribe following structured medication reviews
There are five categories under which you can defend your decision to deprescribe according to SAGE. They are as follows:
- Data collection: Did I collect an appropriate range of data – do I have all the information I need to make a decision?
- Interpretive process: Did I use the data to make a shared decision – did I involve the patient in the decision-making process, and do they understand it?
- Explanation offered: Did my decision support or address improving health as a resource for living? Making sure that you are improving quality of life by stopping medicines that could be causing side effects and may not be useful to the patient.
- Generalisability: Would I have made the same decision for others in the same circumstances?
- Evaluate validity: Did my decision making make a difference for this individual? This should be reviewed at a later point to see if the patient improved or deteriorated.
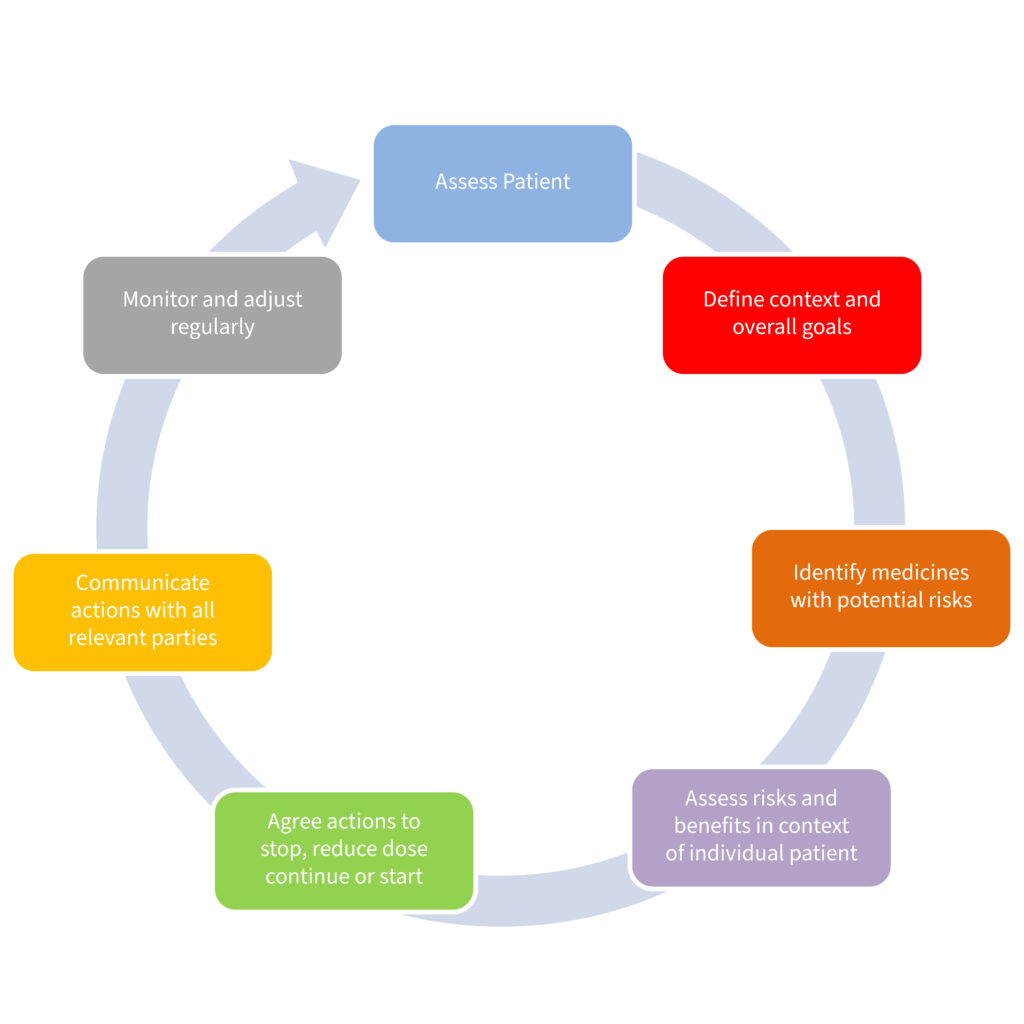
Follow up to deprescribing
There is a follow up and safety netting to deprescribing that was designed by Consultant Pharmacist Lelly Oboh and Professor Nina Barnett. They regard it as a circle with the following points:
- Assessing the patient
- Define context and overall goals – what is important to the patient – quality v quantity of life
- Identify medicines with potential risks
- Assess risks and benefits in the context of the individual patient – is it likely to be beneficial and could it cause harm?
- Agree actions to stop, reduce dose, continue or start
- Communicate actions with all relevant parties and document it
- Monitor and adjust regularly- schedule a follow up consultation with the patient and make sure they know they can contact you if they need to
Further information on structured medication reviews and deprescribing
To find out more about structured medication reviews and deprescribing, you can sign up to one of our FREE webinars. Webinars include case studies so that you can put your learning into practice when you return to your own patients.
In his webinars, Dr Petty also talks about deprescribing anticholinergic medicines and how to identify patients with a high frailty and high anticholinergic score based on the anticholinergic scale. You can then target them for anticholinergic reviews. Opioid and benzodiazepine deprescribing is also covered in our structured medication review webinars. To find the right session for you, head to our training page.





